New leaders are confronting the organization’s years of drift—and trying to reinvent it for a new dental economy. Can they succeed before it’s too late?
By Jerry Markon
LIKE MANY DENTISTS before him, Dr. Arsh Ahuja once viewed the American Dental Association as beneficial for practice owners who needed continuing education and other hard-to-get benefits.
But as he became a practice owner, Dr. Ahuja began hearing complaints from younger dentists. The ADA doesn’t assist with financial planning and student loan repayments, they said, or help navigate the rise of DSOs and other changes roiling the profession. And CE, once the ADA’s domain, is now everywhere.
Today, Dr. Ahuja considers the ADA to be “archaic. It’s usually composed of older dentists about to retire or newer dentists trying to get discounts on their malpractice insurance.
“There are hundreds of online CE courses that are better than what the ADA has,” adds Dr. Ahuja, 42, the founder and owner of a DSO that operates 30 practices in California and New York. “There is no benefit to the doctor for having that membership.”
Asked if he ponies up for ADA memberships for his doctors, roughly 10 percent of whom belong to the organization, Dr. Ahuja replies: “Absolutely not.”
Yet he has not given up on America’s largest dental association. “Everyone is still looking to the ADA,” says Dr. Ahuja, who remains a member. “Are they going to reinvent the ADA so it can cater to everyone?”
Diagnosing the Drift
Dr. Ahuja’s experience embodies the problems—yet also the promise—of an ADA that stands at a generational crossroads. With the organization in the grip of a two-decade membership decline, revelations of recent months have been withering: a financial crisis marked by deficit spending, a draining of ADA reserves and the botched rollout of a new association management system, which led to more than $20 million in budget cuts.
Dentists and current and former ADA officials interviewed by Incisal Edge say the difficulties reflect a deeper struggle to adapt to changes in the profession, from the rise of corporate dentistry to diminished loyalty from younger doctors struggling with student debt.
And in an era when rapid digital communication with members is key, many say the ADA remains bogged down by an unwieldly management structure geared to support the old guard: longtime practice owners.
“The ADA’s current financial problems are less about a single failure and more about long-term institutional drift,” says Dr. Howard Farran, publisher and founder
of Dentaltown, whose June 2025 article calling for reform at the ADA helped publicize the problems. “Dentistry 50 years ago was overwhelmingly private practice. . . . Membership in the ADA was almost automatic. The organization evolved around that reality.”
Over the past several decades, “that enviroment has changed dramatically. . . . At the same time, the governance structures of the ADA remained largely unchanged,” adds Dr. Farran, a regular on Incisal Edge’s 32 Most Influential People in Dentistry list who lands at No. 29 this year.
Reinvention, Not Just Reform
To ensure the future of an organization widely seen as vital to organized dentistry and oral health care, Dr. Farran and other critics are calling for nothing less than a reinvention of the ADA, an overhaul of practices and priorities. Among their ideas: focusing on transparency to rebuild member trust, supporting younger dentists working in corporate environments as well as private practices, consolidating the ADA’s core functions and streamlining the organization’s complex governance structure.
Everyone is still looking to the ADA. Are they going to reinvent the ADA so it can cater to everyone?”
—Dr. Arsh Ahuja
Currently, the ADA has a board of trustees, which is its administrative body with 25 members, including eight officers—along with a House of Delegates. The House is the ADA’s legislative and governing body, with 483 voting members.
The ADA’s new leadership is hearing the call. “Reinvention is necessary,” says Dr. Nader A. Nadershahi, who was named the organization’s executive director in March. “It’s not reinvention of our mission and purpose. It’s about how we deliver value and how we continue to raise the importance of oral health care as critical to overall health and well-being.”
In early April, barely a week after starting the job, Dr. Nadershahi—at the top of this year’s 32 Most Influential list alongside two colleagues—was already considering steps such as “modernizing membership” by piloting more flexible models for providing member value. “It’s important to look at members and where they are in the stages of their careers and in their practices, and how we can best support them,” says Dr. Nadershahi, 55.
Currently, ADA members pay $627 in annual national dues, which recently increased from $570, alongside reduced-rate categories based on the stage of one’s career. Combined with local and state dental association dues, the total cost can run as high as $2,000 in some states.
The ADA says the dues increase, approved in October, was necessary for long-term financial stability. Some dentists contend that the relatively high dues—combined with what they perceive as a lack of value—have helped drive members away.
Another new ADA leader, Dr. Richard Rosato, says he is “trying to create a culture change, a culture of listening,” because he has been frequently told that the organization “doesn’t listen” to its members. “Definitely, yes, the ADA should be doing things differently,” says Dr. Rosato, who became the ADA’s president last October. “We have to listen to members at every level, not just people who have been involved for 25 years.”
 Fighting to Win Back a Generation
Fighting to Win Back a Generation
Another way the new president is trying to change how the ADA does business: focusing on the student loan issue, widely seen as dentistry’s biggest ticking time bomb.
In the One Big Beautiful Bill Act, passed last July, Congress capped the amount of federal dental school loans an individual can take out at $200,000 in a lifetime, a limit significantly lower than the average debt for dental graduates. It’s one of a number of major challenges facing dentistry that have coincided with the ADA’s troubles, including staffing shortages of hygienists and the battle over the Trump administration’s efforts to limit fluoride in drinking water.
On student loans, the ADA recently joined a coalition asking the U.S. Department of Education to adjust the timeline for the changes. “It’s a huge priority; it’s keeping me up at night,” says Dr. Rosato, 57, who is working with the ADA’s credit union to find loans to help students with shortfalls.
Above all, ADA leadership is focused on engineering a resurgence of membership, which has steadily declined since 2007. At its height in the 1940s, around 85 percent of U.S. dentists were ADA members. As of the end of 2025, that had fallen to 51.7 percent, though ADA officials have recorded a slight increase early this year.
“We’ve been trying like crazy to reverse the declining market share,” says Dr. Brett Kessler, the ADA’s president for a year before Dr. Rosato. “Everyone joins the ADA for various reasons—some for advocacy, some for science, networking, CE and on and on. We haven’t been able to boil down a cogent value proposition, an elevator speech that is one size fits all.”
One prominent critic, at least, is impressed: Dr. Bob “Dee” Dokhanchi, an Illinois dentist whose April 2025 LinkedIn post helped expose what he called “years of financial mismanagement, failed oversight and questionable spending” at the ADA. Now, he tells Incisal Edge, “I have confidence in the people in power. I didn’t have that before. They are listening, but the ADA is more than 150 years old. Policies change slowly.”
Dr. Dokhanchi, 60, who is the founder of Dentistry in General, an events, podcasting and media publishing platform, urged the ADA to market more effectively to non-member dentists. “For a dentist to grow a practice, they need to constantly
market to non-patients,” he says. “The ADA is marketing to the choir. Everything that comes out goes to people who have already paid.”
 Difficult, but Not Unprecedented
Difficult, but Not Unprecedented
The ADA’s membership struggles are part of a broader trend of flat or declining membership in professional associations. Sequence Consulting, an Illinois firm that works with such groups, has documented recommended steps to address membership declines—ranging from redesigning websites to bringing in new leadership and rebuilding member value and trust.
The American Diabetes Association, for example, reversed a steep membership decline with changes such as introducing more members-only benefits, simplifying membership categories and pricing, and expanding networking opportunities, according to a 2025 case study. Officials from the diabetes association and Sequence Consulting declined to comment.
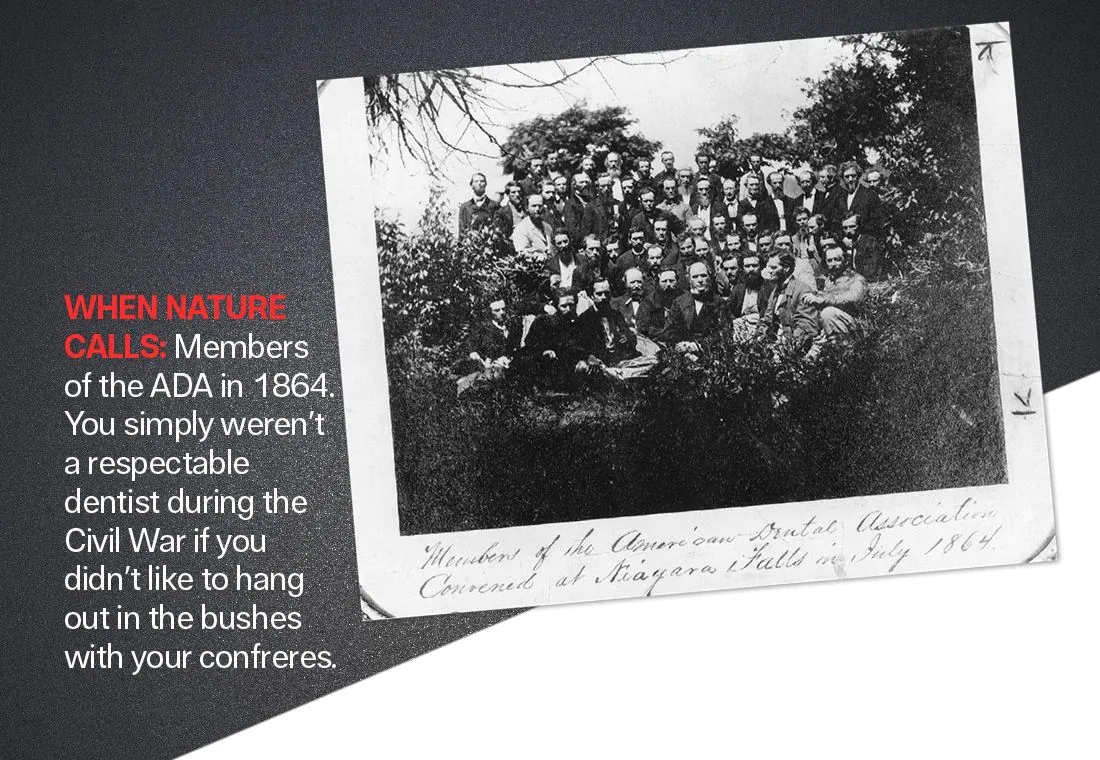
Membership decline was a long way off back in 1859, when 26 dentists met in Niagara Falls, New York, to form the American Dental Association. Growth was the operative word; as recently as the late 1980s, “you almost had to join the ADA,” says Dr. Jeffrey S. Cummings, a dental practice owner in Waltham, Massachusetts.
“If you didn’t participate in your local dental society or become a member, you were looked down upon.”
By 2017, with lobbying expenses having jumped over the previous decade, the ADA was a powerful force in Washington, leading the Washington Post to bestow perhaps the ultimate insider Beltway compliment: The political clout of dentists and their lobbying organization, a Post article said, “rivals that of the gun lobby.”
Today, with 152,000 members, the ADA spends close to $2 million a year on lobbying and is known as a leader in dental science and research. It develops and tests dental products and materials; its trusted Seal of Acceptance helps consumers and dental professionals identify oral care products that meet rigorous standards for safety and effectiveness. The ADA also publishes the prestigious Journal of the American Dental Association.
Yet the membership decline has been building, and by 2021, the ADA Board of Trustees had projections indicating it would continue, while non-dues revenue was also down. The board endorsed a business plan to reverse the downward trends.
As the board would disclose in a series of emails to members in mid-2025, the ADA spent some $142 million from its reserve funds on a series of investments between 2022 and 2025. That drained nearly half of its total reserves.
Revenue fell 6 percent between 2024 and 2025, with the board saying in a July 2025 email to members that its expected revenue growth and cost-saving measures “have not occurred.”
What was by far the largest reserve fund investment, $53 million to finance a new association management system (AMS), went badly. ADA officials said AMS—a centralized system to house member information, process memberships and customize recruitment and retention outreach—was necessary because the previous system was outdated and vulnerable to data breaches.
But AMS’s four-year-timetable was significantly accelerated, causing it to work poorly and run over budget, according to board emails and ADA officials. The ADA wound up taking $27.5 million from reserve funds to cover 2023-24 deficits; officials said last year’s deficit was around $20 million.
The revelations triggered angry online comments from ADA members, some of whom said the developments crystallized concerns that the ADA was mismanaging its finances and had not adapted to changes in the profession.
“People have gotten wiser. Why would I give the ADA $1,000 a year when they don’t represent me and don’t do very much for me?” says Dr. Cummings, the Massachusetts practice owner who dropped his membership last year after 38 years.
Dr. Cummings adds that the business skills required to run a national association elude many of his clinically focused colleagues. “It’s not our natural gift,” he says. “We’re a bunch of dentists.”
Dr. Ahuja, the DSO owner in California and New York, agrees that the ADA “needs to be run like a true business and help younger dentists get the business education that pertains to the changing landscape.” He urged the ADA to assist younger doctors with student loan repayment and practice acquisition skills, while holding more networking events to connect them with retiring dentists.
Others called on the ADA to reform what is widely seen as a bloated management structure, along with the one-year term limit for its president. “The one-year term is a problem because every president comes in with an agenda, and it causes us to zigzag,” says Dr. Kessler, the former ADA president. “I constantly wondered as president who was in charge—me, the board,the executive director or some random member who wanted to know about an
obscure line item in the budget.”
The ADA has taken the short-term step of implementing more than $20 million in budget cuts starting last August—and recently introduced a key longer-term project: the Oral Health 2050 Initiative. Led by Dr. Rosato, it will explore the future of topics such as oral health and wellness, patient payments and cost, and AI in dentistry.
The budget cuts—which include a shifting of some in-person events to virtual; a suspension of some diversity, equity and inclusion programs; and staff reductions—are helping stabilize the ADA’s finances, says Dr. Nadershahi, the new executive director. “The finances are improving,” he says. “That has helped the organization move forward.”
Confronting the Future
James Schulz Jr., 57, the ADA’s senior vice president of government and public affairs, likes what he’s seeing. “I think leadership is on the right path,” he says. “They’re actively sharpening the ADA’s role by defining what we do best and where we bring the most unique value.” As Incisal Edge was going to press, the ADA announced it had hired the consulting firm Vista Cova to conduct “a comprehensive governance and organizational health evaluation,” with a report expected by early 2027.
Dr. Amy Adair, a pediatric dentist who practices in Burke, Virginia, and who has expressed concern about the ADA’s communication with members and its dense leadership structure, is also cautiously optimistic. “It takes a long time to turn a ship, but I do think the ship is trying to turn,” says Dr. Adair, 45. “What the ADA has historically brought to the table has been helpful for dentists. But I think we’re at an interchange where the ADA needs to make some decisions—and that’s going to be a big deciding factor in how helpful the ADA is going to be in the future.”