By Edward Kobesky, Jerilyn Forsythe and McKenzie Kupchik
THE FORCED ISOLATION of the earliest days of the pandemic brought with them a bit of a silver lining, if you squinted hard enough: constant reassessment of the old way of doing things. To some extent, that simply meant a reorganization of dental practices’ daily affairs to compensate for the new normal that had descended without warning. In another sense, though, it helped spark a furious rush of innovation that continues to the present day.
In the pages that follow, our annual review of the previous year in dental innovation, we’ll try to make sense of some of these changes and what they mean for the profession going forward. We’ve highlighted a handful of important people doing innovative work in a variety of aspects of dentistry; taken an in-depth look at evolving practice models; gotten a sense of the modern dental laboratory; taken stock of the exploding market for clear aligners; and much more, including two splendid new inductees to our Dental Innovators Hall of Fame. We also take a deep dive into artificial intelligence: what it is, how it’s already affecting the practice of dentistry and what lies ahead. The profession we all love has, circa spring 2022, become a boiling cauldron of innovation. Here’s a look at the current state of it all.
The Aligner Market
Clear Winners—and New Challengers
Invisalign’s innovation-driven momentum has kept it at the top of this burgeoning market segment.
 ALIGN TECHNOLOGY continues to dominate the clear aligner market—and well beyond, thanks not only to its Invisalign product but also the highly regarded iTero intraoral scanners and exocad CAD/CAM software. While Smile Direct Club continued to face significant struggles in 2021, Invisalign’s model of doctor-led treatment (as opposed to the direct-to-consumer model derided by doctors) was bolstered by continued support among the professional community, as well as patient confidence.
ALIGN TECHNOLOGY continues to dominate the clear aligner market—and well beyond, thanks not only to its Invisalign product but also the highly regarded iTero intraoral scanners and exocad CAD/CAM software. While Smile Direct Club continued to face significant struggles in 2021, Invisalign’s model of doctor-led treatment (as opposed to the direct-to-consumer model derided by doctors) was bolstered by continued support among the professional community, as well as patient confidence.
Impressive financial results aside, Align’s significant investments in developing leading tech are what make it a darling among practitioners. Yuval Shaked, the Phoenix-based company’s senior vice president and managing director of the iTero systems and services business, says Align invests about $250 million annually in product development. Advances in its digital platform during 2021 included the Go Plus system, which supports more complex cases, and the new iTero Workflow 2.0 software, which enables doctors to capture, annotate and share Invisalign simulations or restorative treatment plans digitally.
In September, Invisalign announced a whitening system that optimizes Ultradent’s Opalescence PF formula for use with its aligners and retainers. This makes sense: If patients are going to wear one for the better part of every day, they might as well get the benefits of whitening at the same time. In fact, according to Raj Pudipeddi, Align’s chief product and marketing officer, half of patients ask their providers for whitening during or after treatment anyway. Many offices already advertise their own improvised systems, so being able to offer an Invisalign-approved solution could offer doctors a marketable advantage.
As an innovation-focused company, Align announced that it has awarded up to $375,000 in grants for “scientific and technological research initiatives to advance patient care in the fields of orthodontics and dentistry.” The program has funded about $2.4 million since its inception in 2010. —Edward Kobesky
Innovative People
Dr. Judith Albino and Dr. Bruce Dye
Scientific editors and co-directors of Oral Health in America: Advances and Challenges
IN 2000, then–Surgeon General David Satcher’s Oral Health in America: A Report of the Surgeon General was a landmark work. Its declarations— on the intrinsic connection between the welfare of the mouth and whole-body health, notably— are now common knowledge. Two decades ago, though, the report’s findings were noteworthy.
A team of more than 400 contributors has now published an update to that report. Oral Health in America: Advances and Challenges was guided by the U.S Department of Health and Human Services, the National Institutes of Health and the National Institute of Dental and Craniofacial Research. The 760-page document, published last December, was co-directed and edited by Dr. Judith Albino, a health and community psychologist and president emerita and professor emerita at the University of Colorado’s Anschutz Medical Campus in Denver; and Dr. Bruce Dye, a dental epidemiologist with the NIDCR. Alongside dozens of project team members, the pair shepherded the nation’s understanding of oral health into the pandemic-fixated present.
Many problems first addressed in the earlier report persist. Though tobacco use has continued to wane, the use of vape and e-cigarette products (for both marijuana and tobacco) has skyrocketed. Oral disease continues to disproportionately affect minorities, the elderly, immigrants and people living below the poverty line, and is influenced by factors including the ability to afford healthy food, access to health care and insurance coverage.
Oral Health in America is capped by three principal calls to action: for dentists and health-care workers together to provide integrative care to all populations; to grow, diversify and adequately train oral health professionals; and to reduce systemic inequalities that affect oral health care.
“Drs. Dye and Albino were instrumental in coalescing a variety of expert voices in the creation of this data-driven document,” NIDCR director Rena D’Souza tells Incisal Edge. “NIDCR, and many stakeholders in oral public health, will reference this report for years to come as a compendium of truly valuable research and analysis.” —Jerilyn Forsythe
THE ALIGNER MARKET: DENTSPLY HAS BYTE
 BLOCKBUSTER VIDEO was once the 800-pound gorilla of the home-entertainment industry. Business scholars will note that the company declined not just one, but two opportunities to either buy or join forces with Netflix, among other seismic missteps.
BLOCKBUSTER VIDEO was once the 800-pound gorilla of the home-entertainment industry. Business scholars will note that the company declined not just one, but two opportunities to either buy or join forces with Netflix, among other seismic missteps.
Which brings us to Dentsply Sirona’s January 2021 acquisition of Byte. Perhaps the Charlotte, North Carolina–based giant saw the writing on the wall: that many patients cannot or simply will not seek traditional in-office orthodontic treatment. Rather than ignore this the way Blockbuster ignored streaming, Dentsply seemingly made a pragmatic choice to acquire the direct-to-consumer brand following Byte’s meteoric two-year rise from zero to over $1 billion in annual revenue—without having taken a penny of venture capital.
Will Byte compete with dental practices? Dentsply Sirona insists that’s not the case. “Many Byte customers indicated that they have never had dental work done before coming to Byte,” the company tells Incisal Edge in a statement. “This is the opportunity to bring these patients into a professional dental network and therefore drive growth for dental professionals as well as improve patient care.”
What about practices currently invested in Dentsply’s SureSmile clear aligner system? The company says it doesn’t expect Byte to have a material impact. “Byte complements our SureSmile aligner solution. It is our goal that Byte will increase the in-office treatment for SureSmile.”
The company also clearly delineates between the two: “Byte [is] built on doctor-directed care that provides excellent outcomes for patients with mild to moderate orthodontic needs. SureSmile . . . provides a complete root-to-crown planning solution for our dental professionals.” More specifically, “the goal of Byte and Dentsply Sirona is to expand the market for orthodontic and dental care by connecting new patients with the existing network of Dentsply Sirona and help these patients access quality oral health care.”
Any concern that Dentsply is backing off, even a little, on supporting dentists is contradicted by recent advances. Last year, the company launched version 5.2 for Connect and Cerec. It also upgraded its SureSmile Aligner software. In the pipeline for 2022, the company says it’s “focused on the megatrend of digitalization and its uptake and potential for dentistry, as well as artificial intelligence technology,” which is already being used in its Primescan intraoral scanners. Specifically regarding orthodontics, Dentsply is planning to integrate SureSmile VPro, an at-home High Frequency Vibration (HFV) technology device, to the SureSmile workflow this year. —E.K.
Innovative People
Dr. Chris Ciriello
Cofounder and CEO, Cyberdontics
THE TRAJECTORY of dentistry is clear: From 3D-printed prosthetics to placing supply orders, procedures are becoming leaner, more automated and increasingly digitized.
The automation space is precisely the one Cyberdontics hopes to step into with its patent-pending fully automated drill. The robotics company was founded by Dr. Chris Ciriello in British Columbia in 2017 and seeks to completely automate restorative dentistry—starting with the dental crown. In essence, Cyberdontics is a platform for crowns and fillings that uses images to guide a robotic arm that evaluates, cleans, preps and inserts the filling into the tooth in need.
With our smart drill technology, we reduce the amount of time a patient spends under the drill from over an hour to just a few minutes.”
Cyberdontics claims its drill reduces the time a routine crown takes from two appointments and roughly two and a half hours of patient time to just one visit and 15 minutes. This proposed shift could be monumental, for both the patient—who bears the cost and physical and emotional burden of hours-long chair time—and the doctor. “With our smart drill technology, we reduce the amount of time a patient spends under the drill from over an hour to just a few minutes,” Dr. Ciriello said in a 2018 interview, adding that the “technology increases dentist productivity by 800 percent during crown and bridge procedures, saving them more than 300 hours a year.”
In the United States, at least, research shows that consumers are warming up to the idea of dentistry delivered via robotics (the first entirely robotic dental implant operation was performed in China in 2017). Though Cyberdontics has not yet been approved or cleared by the FDA for medical use, automated restorative procedures might just be available in the operating room sooner than we think. —J.F.
THE ALIGNER MARKET: A Market Ripe for Challenger Brands
 UPSTART ALIGNER BRAND Str8 is the brainchild of Dr. Misee Harris (right), a doctor with a passionate entrepreneurial streak—and the guts to sink 100 percent her own money into a (mostly) vertically integrated startup that she says taps an unexploited pricing niche. “Invisalign does a great job, and so does Byte,” she explains, “but they’re still not accessible to a large section of the population. Straight teeth, even today, are a luxury for the few.”
UPSTART ALIGNER BRAND Str8 is the brainchild of Dr. Misee Harris (right), a doctor with a passionate entrepreneurial streak—and the guts to sink 100 percent her own money into a (mostly) vertically integrated startup that she says taps an unexploited pricing niche. “Invisalign does a great job, and so does Byte,” she explains, “but they’re still not accessible to a large section of the population. Straight teeth, even today, are a luxury for the few.”
A pediatric dentist in Jonesboro, Arkansas, Dr. Harris—a member of the Incisal Edge 40 Under 40 in 2021—hopes to change that with doctor-led clear aligner treatment for what the company says will be one of the market’s most affordable monthly fees. “We want Str8 to be simple, straightforward and accessible,” she says.
Dr. Harris started work on the brand in early 2021, focusing on the clinical side, investing more than $250,000 in her own lab. Then she and her lab techs immersed themselves in CE and partnered with doctors worldwide: “People tend to think that the most advanced knowledge is centered here in the United States, but we learned so much from the international community.”
She and her team developed Str8’s branding while using her practice as a test market. Within a few months of her soft launch, demand exceeded her ability to provide impression kits. But while Str8 will be offered through a network of providers as well as direct to consumer, Dr. Harris says “the patient experience needs to be as close to in-office treatment as possible using telemedicine.” Str8 will cover the cost of an initial dental examination, with all cases reviewed and designed by dentists and orthodontists.
Str8 launched February 15, and Dr. Harris is equal parts realistic and ambitious about going national. “Even if we get 300 more
cases a month, that’s a great start. It’s something we can manage in terms of patient care, but the plan is in place to scale up as quickly as we need to,” she says.
Giving back, too, has been baked into Str8 from the start. Dr. Harris is the founder of Jonesboro’s Louise Hage Medical Center (named for her grandmother), which turns no one away. She hopes to offer more pro bono treatments as Str8 grows. “Perfect smiles are great, but improved smiles can also be life-changing for people. We can’t fix skeletal Class III open bites, but with aligners and bands and attachments, we can do the next best thing and camouflage.” So far, she says, Str8 has been able to treat about 90 percent of cases.
Str8 is minuscule compared to Invisalign, Byte and Smile Direct Club. You can argue that it’s simply using off-the-shelf tech. But that all misses the point. Dollar Shave Club didn’t reinvent the razor blade; it didn’t even invent its own razor blade. Where it succeeded was in challenging the prevailing cost and buying process. That was enough to go from zero to a $1 billion–plus sale to Unilever. Keep an eye on this space, because the next big player in aligners could come from just about anywhere. —E.K.
Innovative People
Dr. Christian Coachman
Digital Smile Design
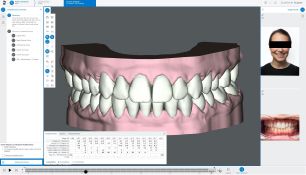
THE CREATIVE MASTERMIND behind Digital Smile Design, Dr. Christian Coachman has been changing esthetic dentistry since DSD’s inception in 2007.
His innovation factory encompasses everything about smile design and reconstruction: the technological education of the practitioner, patient communication, software implementation, delivery of the final smile and a library of information and support available to clinicians.
Dr. Coachman’s immersive three-day residency course empowers dentists to provide an entirely new smile for their patients. Digital Smile Design uses digital design and photography to map and detail smile construction based on facial structure, providing a true-to-life image that a patient can approve before any work begins. Reconstructive or esthetic dental work, of course, is inextricably linked to patients’ emotional response, so lightening that burden increases patient-provider trust.
Using intraoral scanners, DSD captures multiple 3D images and exports them to its signature software, after which countless images of potential teeth and smiles can be laid over the scans, providing a physical model from which to work.
The company’s future, Dr. Coachman says, is to continue to push educational boundaries. “It’s not about individual fancy technologies but how to insert technologies and procedures into smart systems. We’re in the business of connecting dots and simplifying processes,” he says. “Every time we get exposed to a new product, idea or technology, we immediately start to brainstorm about using it. We then try to insert it into a realistic workflow and explore the challenges of implementing it. Based on the implementation challenges, we build our educational programs that hopefully will help professionals implement the idea and benefit from the outcome.”
Fittingly, innovation runs through the Coachman lineage, beginning in the late 1800s with Dr. Coachman’s great-great-grandfather, who is credited with kickstarting the formal practice of dentistry in Brazil. Dr. Coachman’s father founded Brazil’s esthetic-minded Keyes-Coachman Institute and Congress in 1993. The current Dr. Coachman’s triumphs, then, are just the extension of a family tradition. —McKenzie Kupchik
INNOVATIVE COMPANIES AND PRODUCTS:
DENTAL PRACTICE MODELS
One Size Doesn’t Fit All
The practice landscape of the future is less about a small number of dominant behemoths AND more a passel of hyperefficient small fry: fewer Goliaths, in other words, and more Davids.

Bookish dreamer: Dr. Michael Verber, the echt entrepreneurial dentist
PRACTICE MODELS HAVE been evolving since the 1960s. It may be true that factors like rising tuition costs, shrinking insurance reimbursement and changing market expectations have helped fuel the growth of DSOs. However, that’s only part of a far more complex story. Different practice types are innovating in response to realities currently facing both doctors and patients (and sometimes, of course, investors).
Independent dental practitioners, or IDPs, continue to thrive. While practice ownership stands at about 76 percent, according to the most recent figures from the ADA Health Policy Institute, only about 10.4 percent of American dentists were affiliated with a DSO—and in some states, that figure is 1 percent or less.
In fact, looked at another way, IDPs and DSOs need one another. DSOs continue to serve as a training ground for some doctors planning to open their own practices. On the flip side, DSOs are good at bulking up their rosters of affiliated offices by acquiring or otherwise joining with profitable independent practices; it’s easier (and less risky) than developing locations from scratch. Of course, that also presents a big challenge for DSOs: Why should prospering, profitable practices affiliate with DSOs when they’re doing just fine on their own? DSOs therefore hardly have a free ride when it comes to expansion, and the pressure is on to make an increasingly compelling case for themselves.
That said, it’s hard to overlook the power of firms like Heartland Dental, which, in 2021, added 424 new practices in 38 states, bringing its total to more than 1,550. Last year, Incisal Edge reported on Smile Brands’ acquisition of Midwest Dental, which increased its footprint by over 50 percent, to 650 offices at the time. There’s also Aspen Dental, with more than 900 offices. So where’s the opportunity? We talked to three key players, and the answer seems to be: Opportunity is wherever you want it.
Leveraging Independence to Deliver Interdisciplinary Care
Incisal Edge has long highlighted what we call “entrepreneurial dentists,” a category of group practices we believe are defined by some common threads: a single owner or small group operating within an intentionally defined geographical footprint, without grand Wall Street plans but with a strong desire to leverage their independence in unique ways.
Perhaps no organization exemplifies the entrepreneurial dentist like the Verber Dental Group. Based in central Pennsylvania and comprising 12 distinct practices with unique brand identities, the group is headed by Dr. Michael Verber, a self-described “CEO who’s not good with money” who still does dentistry at least three days a week.
Dr. Verber’s current business mission isn’t driven by profit but rather “offering interdisciplinary care within our own ecosystem,” he says. “Our vision is to create a fully functioning dental health system” to address gaps in care, and to exert continuity of care for control over outcomes. To that end, all Verber Group offices are located within a 10- or 15-minute drive from his Specialty Center.
I’m the dreamer, so my leadership team needs to keep me grounded in business reality.” —Dr. Michael Verber
All those offices are owned by their local doctors, who function as managing partners, all of whom “have skin in the game. If they’re not partners, they’re on the partnership track.”
Lately, Dr. Verber has been working to complete a new 15,000-square-foot headquarters and training center that will house the Verber Advanced Dental Institute. He freely admits that neither his dental health system plan nor the educational complex puts business concerns first: “Money was always a distant second for me.”
But that’s key to why he’s creating his own model rather than following another. “We’re more interested in clinical economies of scale than business ones. This is the difference between our DHS [dental health system] and the DSO model.” Dr. Verber credits his executive team with continually distilling his goals into workable business plans.
“I’m the dreamer, so my leadership team needs to keep me grounded in business reality,” he says. “Strictly speaking, every piece of the puzzle I envision may not make financial sense, but they don’t have to—provided they coalesce into a whole that allows us to deliver the level of care we aspire to.” Though he’s quick to downplay his business acumen, it’s clear he has been right far more often than wrong. It’s also proof of how, with the right support, an entrepreneurial doctor doesn’t have to focus 100 percent on business.
“Values-Based Growth”

Pro-ownership: Pete Swenson, Park Dental’s CEO
Park Dental recently celebrated its fiftieth anniversary. What started with two doctors’ early concept of what a group practice could be now encompasses 52 locations throughout Minnesota and Wisconsin. It’s larger than the entrepreneurial dentist model, but nowhere near the market penetration of Smile Brands, Aspen Dental or Heartland. That’s intentional, according to Pete Swenson, the company’s chief executive officer: “One of the biggest roadblocks I foresee for some of the big DSOs is their inability to provide an ownership stake for the doctors, with real leadership opportunities and a voice in the organization’s culture and strategy.”
To my mind, doctor ownership means maintaining control over the things that matter most—clinical, hiring, culture—while freeing up resources by outsourcing other functions. Day-to-day autonomy to practice dentistry and to shape the dental office itself has always been a pillar of the Smile Brands philosophy.” —Steve Bilt
While Park Dental is sticking steadfastly to its model of “values-based growth,” as the company characterizes it, it has also been quick to adapt to the changes imposed by the pandemic. The company has reduced the amount of administrative space it leases by half. After transitioning to remote work wherever possible in 2020, support teams will remain remote for the foreseeable future. Says Swenson, “Our challenge is to balance remote work with the right mix of in-person interaction” so that the “collaboration and connectiveness” central to Park’s culture can continue.
To that end, Park Dental has devised its own clinical and business data dashboards, providing insight it calls “well beyond the static-type reporting [of] most systems” and which informs most operational decisions. On the patient side, it puts all available hygiene appointments online, which increased access and reduced the number of open or unused appointments.
Analytics software helps Park schedulers zero in on patients who are statistically most likely to miss their hygiene appointments, delivering a 30x return on investment. Combined, these tech solutions help make the most of highly trained team members, which “couldn’t have come at a better time,” Swenson says, “as the dental profession struggles to fill open hygiene and dental assisting positions.”
Park Dental has clearly avoided growth strictly for growth’s sake. It aims for synergistic partnerships with dentists who want to grow their practices and be onboarded seamlessly. Not surprisingly, it’s also finding more dental grads open to a different path to practice ownership than doctors in the past. “They’re embracing the idea of group practice,” Swenson says. He acknowledges that student debt is an influencing factor, but also believes Park’s success is “in recognition of the advantages of practicing in a group, especially in a setting like Park Dental, where the doctors participate in the leadership of the group and can have an ownership stake to share in the growth and success of the group.”
Looking ahead, Swenson says the increasing complexity of the oral health business is likely to benefit group practices like Park Dental and make them more attractive for certain doctors. He cites regulatory compliance and the current payor landscape. “Group practices like Park Dental are better positioned to navigate all these issues, and at the same time we’re also able to approach the interesting and innovative new technologies developing in areas such as augmented clinical intelligence.”
Ownership’s new meaning

Clinicians in charge: Smile Brands CEO Steve Bilt
As for the core appeal of different practice models, the more things change, the more they stay the same. Steve Bilt, CEO of Smile Brands, says the basic idea of “doctor ownership” remains as valued as ever, but it’s evolving. “To my mind, doctor ownership means maintaining control over the things that matter most—clinical, hiring, culture—while freeing up resources by outsourcing
other functions” and that “day-to-day autonomy to practice dentistry and shape the dental office itself has always been a pillar of Smile Brands’ philosophy.”
Ownership in Bilt’s firm lets “doctors to choose their work environment as it relates to equity participation. We’ve found that some clinicians greatly prefer to work as an associate in a group, maintain flexibility—mobility and capital liquidity—and have unlimited earning potential. Others are certain that they want a hard equity investment in the location where they’re practicing, and others want to invest at the group level.”
Bilt calls the last two years a “period of dislocation” during which connection at Smile Brands is maintained through increased internal communications, town hall meetings and in-person field-level conversations. Participation in continuing education has increased exponentially, and as a result, offices have “greatly expanded their offerings, which has increased accessibility, convenience and affordability for their patients.”
NEW Models, NEW CHOICES
Business models may be changing, but practice ownership seems like a smarter bet than ever, if only because of all the freedom—and options—it affords. Bilt thinks the smart play is for practice owners to partner with a DSO “mid-
career while maintaining a substantial ownership stake and driving growth going forward.” Park Dental’s Swenson is confident that “the trend for larger group practices will continue as others realize the value that a group of like-minded professionals can bring.”
Dr. Verber says being fiercely independent perfectly suits someone who, like him, is “driven by the love of dentistry, where the business side comes second.”
Any way you slice it, while business realities are the primary force driving the evolution of traditional practice models, technology and human ingenuity are making this evolution possible—and opening more, albeit different, doors throughout doctors’ careers. —E.K.
Innovative People
TO BE DETERMINED
Head of dentistry, Walmart
BREAD, MILK, EGGS, pajamas, tire changes: Especially in rural areas, what don’t people rely on retail behemoth Walmart for? The next item on the list: tooth care. Walmart launched its first dental location in Dallas, Georgia, in 2019, inside its 10,000-square-foot Health Center.
The company’s dental efforts have been halting a bit over the last couple of years, however. Sean Slovenski, president of Walmart Health, left the company in August 2020 to head a diagnostic testing and immunization outfit called BioIQ; Dr. Roshan Parikh, the company’s inaugural head of dentistry, departed in March 2021; and Dr. Thomas Van Gilder, its first chief medical officer, followed suit that May. (Incisal Edge profiled Dr. Parikh in our 32 Most Influential People in Dentistry issue in 2020, citing his plans for Walmart Dental.) What’s going on?
Most who left were disappointed that ‘changing the world’ wasn’t going to happen on the timeline they imagined. They weren’t Walmart lifers and have moved on.”
“I appreciate that dentistry is unique to Walmart Health’s offering, but the success of that line of business is inevitably tied to the clinics,” James A. Gardner, an Boston-based retail consultant who follows Walmart closely, tells Incisal Edge. “Why were they adrift through 2021? Shifting priorities. Walmart’s board never fully embraced the clinics, and then the pandemic tilted them into survival mode—a fight for their life versus Amazon and online shopping.” Citing Slovenski and others, he adds, “Most who left were disappointed that ‘changing the world’ wasn’t going to happen on the timeline they imagined. They weren’t Walmart lifers and have moved on.” (Dr. Parikh, who this February was named president of New York City–based DSO Dntl Bar, declined to comment when contacted by Incisal Edge.)
Walmart is hardly the only business forced into a pivot by the pandemic, of course.
And once the board decides to name a successor to Dr. Parikh, that person will instantly become one of the most important people to dentistry’s future. Gardner doesn’t put it past Walmart to rekindle its interest in oral health. “I admire Walmart’s vision but am not bullish on their short-term [dental] prospects,” he says. “They’re best watched with a two- to four-year horizon as they find a new way forward.” —M.K.
INNOVATIVE COMPANIES AND PRODUCTS:
LAB REPORT
Nothing Left to Chance
From outside audits to strict internal processes, Argen uses multiple layers of accountability to stay ahead of what customers demand. The last two years in particular have seen the company ramp up automation, planning and process validation.

Machines learning: (From left) ArgenIS Custom Abutments are five-axis precision-milled and compatible with 15 leading implant systems; zirconia milling in Argen’s facilities
ARGEN BEGAN AS A small family business in 1963, growing to become the largest manufacturer of precious dental alloys in the world in 2005. By 2011, the company opened Argen Digital, and today, its 140,000 square feet of total production space run 24 hours a day, six days a week. Incisal Edge recently caught up with Julie Woolf, the company’s co-owner and chief operating officer.
On being accountable for continuous improvement: “We just passed our second annual Medical Device Single Audit Program audit. It allows an annual regulatory audit of our medical device manufacturing quality management system to ensure we meet the requirements of five regulatory authorities: [those of] Australia, Brazil, Canada, Japan and the USA. As a major focus of the audit, MDSAP requires demonstration of continuous improvement year after year, which Argen has proven to satisfy. Our operations are constantly evaluated to make certain we remain agile and lean. On top of this, we have unique protocols and processes for bringing new products to the market, as well as analyzing all current offerings for potential optimizations.”
On automation and innovation over the last 12 months: “Our ArgenIS Implant Systems operation uses custom-built, five-axis FANUC [robotic] Rotodrills, six-axis FANUC robots and software that work together to streamline and automate our abutment milling process. Our Argen Clear Aligner manufacturing is supported by a state-of-the-art MES/SCADA system that provides real-time visibility, control and scale to our manufacturing. We have also invested heavily in argen.com, with a focus on allowing customers to easily upload files, manage their orders, payments, 3Shape dongles and more, all in one place. For standard and digital orders, users can submit orders online, reorder items with the click of a button, view product technical sheets, track packages and manage returns and cancellations.”
On the increasing importance of digital workflows: “Doctors are performing more digital impressions, case approvals and prescription forms, as well as submitting invoices and payments electronically. Argen continuously improves our digital workflows to help our dental laboratory customers meet the needs of their doctor customers. For example, our dental lab customers now simply upload a digital file, and the case is on our production floor almost immediately. Our Argen Digital manufacturing center houses a fleet of more than 100 3D printer and milling systems, supporting a 24-hour turnaround time.”
On adapting to supply chain and other business disruptions: “The expectations of our laboratory customers have become more dynamic. We’ve been able to satisfy them by emphasizing our focus on flexibility and communication with our customers. We’ve created personalized solutions in many circumstances to help them succeed. Additionally, we’ve been working much more closely with our suppliers to ensure we can fulfill orders as expected. Overall, we continue to see that honest communication, integrity and transparency are key to our continued partnerships.”
On planning ahead: “We believe that the next few years will continue to see integration between software and technologies that Argen and our partner laboratories use. As a result, we’re continuously researching potential efficiencies, automations and integrations, and analyzing the benefit they would have for our customers’ workflows. In addition, we conduct market research and customer surveys, as well as regularly communicate with our customers, to ensure we fully understand the processes of our partner laboratories and how we can continue to make their lives easier.” —E.K.
DEVELOPING-WORLD DENTAL SCHOOLS AND THE PANDEMIC
SCHOOL’S OUT, ONE YEAR LATER
Dr. Yasir Israr follows up his prior report (Incisal Edge, Spring 2021) on the developing world’s rocky shift to online education in response to the pandemic. What has changed for the better, where does progress remain stalled—and is optimism about the future warranted?

Artist in residence: Dr. Yasir Israr
ALTHOUGH MUCH OF the rest of the world had an armamentarium in place to adapt to the challenge of Covid-19 lockdowns—shifting much of life and academia online with relative ease—developing countries were slower to react, getting virtual education off to a shaky start. They encountered many setbacks: a limited budget for technology, as well as a generation gap to overcome, since senior dental-health instructors were neophytes to this kind of teaching. Adaptations had to be made slowly over the course of the lockdown.
As of January 2022, one might have thought such countries—my native Pakistan among them—had made considerable progress over the preceding two pandemic years. However, our team conducted multiple online surveys of undergraduate dental students throughout the country about their learning experiences, and the results were mostly negative. The majority said they could detect little beneficial change in the dental education infrastructure.
The problem was if anything more acute among postgraduates. An orthodontic resident, I saw significant setbacks in my program. Unlike other specialties, orthodontics relies on 18 to 24 months of consistent patient follow-up, with close monitoring of treatment progress. During the first nine months of the pandemic, many patients simply dropped off the grid, having lost interest in pursuing treatment, while others reported back after long periods with broken appliances in tow. This was deleterious to trainees’ residencies: Many had to start fresh with limited time to repair the resultant damage. Stress increased.
Developing countries were slower to react, so virtual education got off to a shaky start. Adaptations had to be made slowly over the course of the lockdown.
As I write this, the Omicron variant is bringing about another partial lockdown in dental education in various areas around the world. However, most educational institutions are now somewhat prepared for it. That does not negate the fact that, as a developing country suffering from inflation, Pakistan has a shortage of suitable internet connections and tech devices for all students.
Looking forward from the current moment, there does seem to be some optimism in the air, given that we now know vastly more about Covid-19 and the coronavirus variants: how they affect people, how best to safely treat them. This is light years ahead of where we were during the panic-induced treatment and isolation protocols of 2020. Can developing-country dentists and specialists consolidate these gains and start to undo some
of the damage of the pandemic’s earliest months? That’s the question that must guide us for the rest of 2022 and beyond.
DR. YASIR ISRAR is a resident orthodontist at Sardar Begum Dental College in Peshawar, Pakistan, and an editor for the Italian Journal of Dental Medicine. Follow him on Instagram @dr_yasirisrar.
Innovative People
Dr. Thomas Hirt
Chief technology officer, Ivoclar
DR. THOMAS HIRT’S writ at Ivoclar extends to the development and eventual success of countless innovative products, including a trio that notched honors this year in The Dental Advisor, among others.
With our broad product portfolio, from scanning to the final restoration, we see a lot of potential to support our customers and their patients’ needs.”
That publication’s “innovative company of the year” for 2022, Ivoclar, which is headquartered in Schaan, Liechtenstein, received commendations for its Bluephase PowerCure curing light; VarioLink Esthetic LC light- and dual-curing luting composite; and Monobond Plus universal quick-acting no-refrigeration primer. But there’s more: namely Ivotion, its digital-denture solution. “We achieved something most people considered impossible,” Dr. Hirt says—a great leap forward in speed and efficiency that will change removable dental prosthetics going forward.
The good doctor also cites e.max ZirCad Prime and e.max Prime Esthetics as products of pride, “in the sense that we developed a new production technology for zirconia that gives us more [shade and translucency] options for the future, and that combines esthetics and strength in the best possible way.”
Looking ahead, Dr. Hirt says “chairside blocks, a redesigned filling material with a new level of esthetics and simplicity [Tetric Prime Esthetic and Tetric Powerfill] and 3D printing solutions” are all on the docket for the team he supervises. “With our broad product portfolio, from scanning to the final restoration, we see a lot of potential to support our customers and their patients’ needs.” —M.K.
Doug Hudson
Cofounder and CEO, Tend Dental
IS IT POSSIBLE to make going to the dentist sexy? This, we imagine, was Doug Hudson’s million-dollar question back in 2018, when he started brainstorming a consumer-centric dental office. Or, more precisely, his $36 million question, as that’s how much he and his cofounders would later raise in Series A funding to realize their innovation: Tend Dental.
Tend, with its high-tech accoutrements, modern-chic aesthetics and patient-first business model, opened its first spa-like office in Manhattan’s Flatiron District in October 2019. (Hudson was CEO of Smile Direct Club from 2013 to 2017.) The space received considerable attention for its appearance and offerings—such as patients’ ability to tune into Netflix via Bluetooth Bose headphones while in the chair; state-of-the-art equipment that minimizes both pain and noise; paperwork that could be filled out all online in advance of an appointment; and even exotic-flavored polishing paste (vanilla, jasmine and something called “aquatic”). Instagram-worthy, in other words.
In addition to those creature comforts, Tend Dental also touts a value system based on transparency for the customer. Yes, the “Brushery,” a pre-procedure powder room for patients to brush their teeth, is stylish enough for some social media love. But patients also know how much they’ll pay even before they arrive. Tend’s website has a simple tool that lets patients check if their exam will be covered by insurance. Its dentists’ compensation, meanwhile, is based on a salary-and-bonus pay scale, rather than on volume.
Tend Dental might have begun as a headline-grabbing startup, but the family of practices now has 21 locations as far north as Boston and as far south as Atlanta. Last April, the company raised an additional $125 million in funding (bringing its total to $198 million), and it plans to open many more locations across the U.S. —J.F.

Incisal Edge is proud to welcome two new inductees into this celebrated group for 2022.
DENTAL INNOVATORS HALL OF FAME
 EDWARD F. ROSSOMANDO, DDS, Ph.D., MS
EDWARD F. ROSSOMANDO, DDS, Ph.D., MS
Founder and President, Center for Research & Education in Technology (CRET)
IT’S WELL-KNOWN that significant gaps exist between what students learn in dental school and the realities of everyday practice. Those gaps have widened in recent years, perhaps most significantly by the unprecedented pace of technological progress. It’s one thing to acknowledge the ever-louder concerns of dental students; it’s another to actually do something about it.
Dr. Edward F. Rossomando not only did something—he also developed a vision for making it happen, then rallied the biggest, most powerful players in oral health-care technology around it. Dr. Rossomando is the founding father of CRET: the Center for Research & Education in Technology, dedicated full-time to introducing the latest technology into dental curricula. Since 2004, the group has worked to align the goals of dental academic organizations and the dental industry to serve the interests of students and, by extension, the patient populations they treat following graduation.
CRET’s main mechanism for accomplishing this is developing Innovation Centers at schools like California’s Loma Linda and the University of Missouri–Kansas City, among others. You’d think it’d be a no-brainer—free technology!—yet CRET has faced skepticism from the start. “There are two extremes,” Dr. Rossomando says. “On one hand, some schools can’t wrap their heads around the idea that CRET will provide them with more than $1 million worth of equipment as long as the school agrees to allow its students to provide care in the Innovation Center for a minimum of two weeks. On the other hand, some schools can provide this equipment for students and see no need to apply to CRET for an IC award. So we work with those schools that want us—and in most cases, the award for an IC goes to a school with a dean who has an inquiring mind.”
As a prominent researcher and academic, Dr. Rossomando was, in some ways, the ideal person to carry the torch for CRET. “Having been a professor at a dental school for 44 years, I knew the mindset and spoke the language of academics.” But he admits that when it came to dealing with corporations, his “researcher mindset” made it difficult to understand those in the business world. He struggled with the principles of entrepreneurship and the process of turning lab advancements into marketable products, despite having significant successes that yielded patents being issued and businesses formed. “It was a hard lesson to learn, but companies don’t want to hear about your latest scientific achievement; they want to know if they can sell your discovery.”
To broaden his perspective, around 2000, he went back to school for a master’s in technology management. This was about the same time the digital revolution reached dental schools. “Unfortunately, the existing dental faculty didn’t know anything about this technology,” he says. “If a company gave equipment to a school, the schools didn’t know what to do with it. For example, one prominent dental company tried simply giving the equipment away, and they found the schools took it but never used it. After many dental companies reported the same experience, it was clear that another approach was needed.”
A turning point, he says, came in 2003, when he had lunch with Carl Bretko, then-president of DentalEZ. “Carl said, ‘We develop all this amazing tech, but schools are slow to adopt it.’ ” By the time the midday meal was over, the two had roughed out a plan to solve a marketing problem on the manufacturer’s side—and an education problem on the schools’ side.
“Fortunately, by this time, I was able to cultivate my inner salesperson. Working with Carl, we were able to go out and recruit like-minded companies.” He also credits Patterson Dental’s Grant Gerke, who helped secure seed money to get CRET on its feet. “One of our biggest challenges at the start was that dental companies are very competitive, so figuring out how to make them work as collaborators was part of getting traction.”
Fast-forward to 2022, and several dental schools are in the process of opening CRET Innovation Centers. Meanwhile, the West Virginia University School of Dentistry opened the Dr. W. Robert Biddington Center for Dental Innovation in 2017, and the University of Mississippi opened the Regions Center for Research and Education in Technology Innovation Suite in 2019. To date, 32 dental companies have signed on as CRET members.
Although he has retired from full-time academics, Dr. Rossomando remains president of CRET and devotes much of his effort to encouraging applications for CRET awards. “I target schools with an ‘early adopter’ approach. I expect about 6 or 7 percent of dental academics will be early adopters, and 6 or 7 percent are laggards,” he says. “My goal is to increase the number of early adopters to 25 percent. If I can do that, I’ll be happy. Until then, I’ll keep trying.” —E.K.
 JOHN A. MOLINARI, Ph.D.
JOHN A. MOLINARI, Ph.D.
Prolific and transformative dental infection-control researcher, professor and author
DENTISTRY’S PREEMINENT academic voice in asepsis and infection control emerged not from the Ivy League or a well-funded laboratory. Dr. John A. Molinari is widely credited with playing a defining role in developing infection-prevention standards in response to the AIDS crisis. His work took place at the University of Detroit School of Dentistry, which was only beginning its evolution into the Detroit Mercy Dental we know today.
Back in 1976, “high-profile outbreaks like Ebola and Legionnaires’ disease were in the news, and people were taking notice of infectious disease—but not so much in dentistry,” he recalls.
The then-33-year-old Dr. Molinari was invited to join the school in 1977 from his faculty post at the University of Pittsburgh, where he had earned a Ph.D. in microbiology. While some thought it was hardly the safest career move, he characterized it as “an adventure and a challenge,” an opportunity to build something from scratch. “I thought about it and decided to go for it. Luckily, the dental faculty in Detroit accepted me early on. I also had good mentors and collaborators, since I was starting with a blank page.”
High-profile outbreaks like Ebola and Legionnaires’ disease were in the news, and people were taking notice of infectious disease— but not so much in dentistry.”
Concern over infectious diseases was building at the Detroit school. However, as in virtually all teaching institutions (not to mention dental practices), infection control was lagging the emerging threats. “Hepatitis B was the big deal at that time, yet no one was using gloves,” Dr. Molinari says.
Medical and early dental research made it clear that if you could protect against Hepatitis B, the same protocols would be effective against other bloodborne threats. He started teaching that line of thinking. “The school quickly embraced it. Our hygiene department led the charge for gloves in 1980, and we got them. It was a good thing, too: By the early ’80s, we were seeing drug addiction and all kinds of risk factors in our patient population.”
When Merck introduced the first Hepatitis B vaccine in June 1982, Dr. Molinari was first in line at the school to receive it, followed by his students. “We went to the administration and said, ‘We want the vaccine for our students.’ I think Detroit was the second dental school in the country to introduce it. It was not required, but students listened to the science and received it. Many dental school faculty also got it.”
The emergence of AIDS focused the health-care community on infection control. By that time, basic protocols could be relatively easily applied to AIDS prevention. Dr. Molinari became a go-to lecturer who was also widely called upon to share his expertise by media outlets like the New York Times, effectively distilling complex microbiological science for mass audiences. “I just love to teach,” he says. “Passing knowledge is a great privilege.”
He has published more than 500 articles, chapters and abstracts on microbiology and immunology. He’s a founding member of the Organization for Safety, Asepsis and Prevention (OSAP) and coauthor of the 1991 book Practical Infection Control in Dentistry. After retiring as chairman of the Department of Biomedical Sciences at Detroit Mercy, he became director of infection control for The Dental Advisor. “I loved it. We had the necessary research equipment and were able to work on and evaluate new technology and products. It all fed into everything from my microbiology background and research experience.”
Now 77, Dr. Molinari says the burgeoning anti-science movement spurs him to keep going. “If I can help, then I need to. I tell groups to look around; some of you wouldn’t be here if not for the vaccinations your parents and grandparents had. Plus, SARS-CoV-2 will not be the last big threat. There are always outbreaks emerging. Dentistry had already adapted to contact and droplet transmission precautions many years ago, and now we’ve adapted to airborne precautions. We don’t need to reinvent the wheel, but we can’t go backward.”
Naturally, Dr. Molinari is also committed to encouraging the next generation. “I tell young people, you need to have a passion. Eventually, you can look back and say you accomplished something.” His own self-summation is characteristically modest: “I like to think I made a positive contribution.” —E.K.
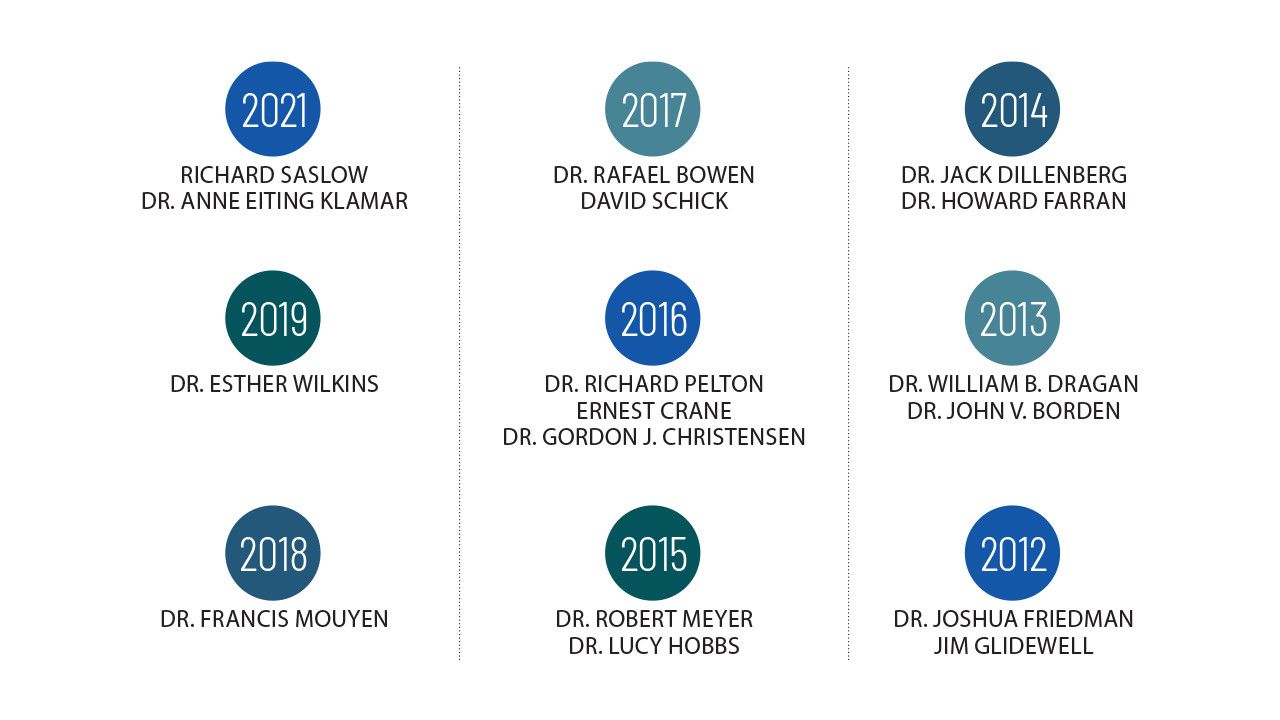
HALL OF FAME: THE INDUCTEES
A decade of worthies—pioneers, inventors, researchers, academics, clinicians and pathbreakers—whom we’ve chosen to elevate to the pantheon of the dental profession. For more information about each individual below, please see IncisalEdgeMagazine.com.
Innovative People
Zhaohua “Emma” Liu
Senior product manager, Carestream Dental
IT’S A SAFE BET that few people in the industry have helped further the evolution of the intraoral scanner over the last decade or so than has Zhaohua “Emma” Liu. Her efforts have helped bring efficiency, an improved patient experience and, yes, innovation to this important segment of the dental market.
Carestream’s growing portfolio of elite scanners is scheduled for acquisition by Envista Holdings for $600 million, a deal set to close at some point before or during the second quarter of this year. Envista, owner of more than 30 dental brands, is focusing on digital workflow as part of its strategic move, says Envista’s CEO, Amir Aghdaei. “This acquisition further enables our purpose of partnering with dental professionals to improve patients’ lives by digitizing, personalizing and democratizing dental care,” said Aghdaei, a fixture on Incisal Edge’s annual 32 Most Influential People in Dentistry list, in a statement.
Carestream, previously known as Kodak Health Group, began to dominate intraoral scanners nearly a decade ago with the launch of the CS 3600. Its newest product might best be described as the (literal) sports car of scanners: the CS 3800, a device whose two-and-a-half-year gestation was conducted in concert with Studio F.A. Porsche, the Austrian design studio whose remit has expanded far beyond its origins with the iconic automaker.
The wireless CS 3800 offers Wi-Fi-enabled support. It’s small and 20 percent lighter than its predecessor. The handheld CS 3800 is designed to lie securely in the user’s palm and conveniently allows for the digital model to move in tandem on the screen, obviating the need to reposition a mouse during scanning. The accompanying software, ScanFlow, provides a four-step guided process, as well as “edentulous scan mode,” which captures a full-arch scan, combining soft tissue in-vivo scans with impression scans. It’s a favorite among her colleagues, Liu says: “It’s a great scanner, easy to use because of the wireless connection and quick, smooth scanning. In our lab, everyone likes to use it. It’s so easy, from hardware setup to actual scanning.” —M.K.
By Kristina Libby
Get Smart! Forget Don Adams and his shoe phone: Artificial intelligence is already transforming the daily practice of dentistry, and its influence will only grow in the years ahead. What is dental AI, though? “It’s not the Terminator,” says one key developer. “It’s more like Siri.” And it’s bound to help practitioners with patient retention, diagnosis, treatment acceptance and the rigors of insurance claims. Brave new world? Sure. But one offering vast improvements in efficiency and oral health overall. Here’s a primer.
 ASK ANY HUNDRED DENTISTS how they think artificial intelligence might change the way they practice, and you’re likely to receive 98 looks of dismay. The wellspring of that emotion could be many things: dread over what lies ahead, disbelief that dentistry will be affected in any way by AI or simply exhaustion from merely thinking about the profession’s post-pandemic future.
ASK ANY HUNDRED DENTISTS how they think artificial intelligence might change the way they practice, and you’re likely to receive 98 looks of dismay. The wellspring of that emotion could be many things: dread over what lies ahead, disbelief that dentistry will be affected in any way by AI or simply exhaustion from merely thinking about the profession’s post-pandemic future.
“Dentists likely do not understand how AI is affecting their business already,” says Wardah Inam, CEO of Overjet, the leading provider of dental AI software, founded in Cambridge, Massachusetts. “We are interacting in an AI environment all the time.” Indeed, recent studies have shown that AI tools are now more consistent than human dentists in diagnosing tooth decay from bitewing and peripheral radiographs. Meanwhile, developments in diagnostics, patient treatment plans, prosthetics and orthodontics, oral pathology, insurance processing and prediction analysis indicate that AI will be instrumental in reducing doctors’ workloads, improving patient trust and boosting proactive patient care.
That actually sounds . . . good, right? Dentistry’s reputation as a hidebound industry resistant to change is nowhere near as pronounced as it used to be, and in any case resistance is probably futile: Within the next 10 to 20 years, experts say, the incorporation of AI will dramatically shift both back-of-house operations and chairside interactions. This will largely occur through great leaps in innovative technologies like “smart” remote monitoring devices—enabling dentists to keep tabs on their patients without having to schedule an office visit—and more mundane improvements such as greater efficiency when filing insurance claims and inputting data into patient records.
AI is not the Terminator—it’s more like Siri. Siri has a lot of limitations. It will not take over our lives.” —Wardah Inam
Dentists will likewise see a rise in companies and services that use AI to improve the dental experience for doctor and patient alike. It will “change how we interact with everything,” Inam says. “We don’t care how it works. We care more about outcomes.” Such progress can be disorienting, but it behooves any clinician to begin to build what you might call “artificial intelligence literacy.”
 WEB SEARCHES AND CONFERENCE CALLS
WEB SEARCHES AND CONFERENCE CALLS
“Artificial intelligence” itself is a term often used to gather a number of related topics under one umbrella. Hollywood’s fictionalized depiction of AI often dramatizes its potential in ways that can seem threatening, leading many to fear some sort of malicious anthropogenic technology with the potential to overthrow and enslave the human race. Inam urges equanimity. “AI is not the Terminator—it’s more like Siri,” she says. “Siri has a lot of limitations. It will not take over our lives.”
Most AI applications in dentistry won’t even be evident from the start. Currently, algorithms and machine learning are used in a number of products consumers rarely think about. Your web search is powered by AI. When you use conference-call software, AI is responsible for the clarity of the call. AI also helps manage complicated shipping and logistics supply chains that help stock inventory and manage assets. (Consider how much worse today’s supply-chain disruptions would be without it.) Often, AI is just under the hood of your favorite technology or product, silently going about its business to make everyday activities run more smoothly.
Fluency helps, though, whether you’re a shipping coordinator at a major port or a general-practice dentist in a small town. Companies in the business of helping dental practices transition to AI augmentation traffic, generally speaking, in four primary concepts:
Artificial intelligence is the notion that machines will someday be capable of performing human cognitive tasks. Coined in the 1950s by computer and cognitive scientist John McCarthy, who was focused on what he called the “science and engineering of making intelligent machines,” the term has now become shorthand for a vast number of sub-concepts.
Machine learning (ML), one such, uses vast amounts of data to develop statistical patterns that can eventually predict future behavior and help sharpen AI’s performance. Neural networks are a type of machine-learning model that outperform standard ML algorithms on complex data such as images or language. We typically discuss “artificial” neural networks (ANN) and “convolutional” neural networks (CNN). Artificial neural networks are able to solve problems too complex to be solved conventionally. They’re useful in diagnosis of disease, biomedical identification, image analysis and data analysis. Convolutional neural networks can be used to read dental records and detect and record teeth—particularly useful in forensic dentistry or on mission trips when patient records might be nonexistent.
(The U.S. military, perhaps unsurprisingly, is one of the leading exponents of AI in medicine. Last November, Dr. Hassan Tetteh, the man in charge of the Defense Department’s Joint Artificial Intelligence Center, told the Wall Street Journal that his organization has “created algorithms so that pathologists can interface with the slides, devising new models to detect cancers such as prostate, colon and metastatic breast tumors, with greater precision and accuracy.”)
Finally, deep learning is a machine-learning model specific to neural networks that uses mathematical operations to enhance learning, and making inferences from, complex sets of data—dental imagery, say. A 2009 study conducted under the auspices of the National Institutes of Health’s National Center for Biotechnology Information used artificial neural networks to build a model capable of predicting toothache by uncovering associations between toothache and daily brushing frequency, brushing time, use of floss, brush replacement frequency and factors such as diet and exercise.
AI is poised to enact profound change across the field of dentistry. We will see dramatic increases in accuracy and transparency, improved patient care and automation on a variety of levels.” —The Dental AI Council
Much more recently, a 2019 research paper reviewed in the medical journal The Lancet showed how deep learning offers considerable promise for medical diagnostics. Based on 14 studies conducted between 2012 and 2019, the review found that deep-learning models’ diagnostic performance was equal to that of health-care professionals. This will only continue to improve as these models become better able to scale up. Fear not, though: These tools will help augment your dental practice. They’re not coming for your job.
The Unique Dental Practice
In recent decades, dentists have adopted a number of technologies to improve their daily practice: business-management software, radiographs and much more. A side benefit of this adoption has been the generation of large amounts of data relating to patients’ care and overall oral health. Indeed, dentistry’s relatively limited scope (in terms of the physical area being tended to and the range of clinical outcomes) makes dental practices ripe for AI incorporation.
Why? Well, consider some of the factors that make a dental practice medically unique:
- Imagery is a central aspect of all dental practices.
- Imagery is routinely accompanied by clinical records, general and dental history and medications.
- Many of the same conditions (apical lesions, periodontal bone loss and more) are relatively prevalent across a given patient base.
These large, cohesive “data lakes” help scientists develop models that can integrate and cross-link data to improve diagnostics, predictions and decision making for both patient and clinician. This is where AI-based dental companies are generating the next wave of innovation.
All this promise and potential, though, is not without pitfalls. As such, a group of scientists and specialists recently formed the Dental AI Council (dentalaicouncil.org), a Los Angeles–based organization dedicated to better understanding the opportunities AI presents.
“AI is poised to enact profound change across the field of dentistry,” the group’s mission statement asserts. “We will see dramatic increases in accuracy and transparency, improved patient care and automation on a variety of levels.” The industry overall, though, is divided over which AI tools are the most beneficial and whether enough research has been done on the tools already making their way into practices nationwide.
Dentists shouldn’t care about whether it’s AI or not—they should care about what’s in it for them.” —Wardah Inam
AI Tools, AI Benefits
 A growing number of companies have recognized the potential for dental AI improvements, launching (and planning to launch) market-ready technologies for immediate daily practice use. These include industry leaders (Henry Schein One, Overjet) and upstarts (Pearl, Vida Health, OrcaAI, Denti.ai) alike.
A growing number of companies have recognized the potential for dental AI improvements, launching (and planning to launch) market-ready technologies for immediate daily practice use. These include industry leaders (Henry Schein One, Overjet) and upstarts (Pearl, Vida Health, OrcaAI, Denti.ai) alike.
“Dentists shouldn’t care about whether it’s AI or not—they should care about what’s in it for them,” Overjet’s Inam says. This means maintaining a clear focus on how AI can help improve the dental experience for both patient and practitioner. In the current phase, the focus is largely on improving chairside care and the patient experience between visits, and back-office processing and efficiencies.
Diagnostic tools are one key component, helping ensure that dentists see a complete picture of a patient’s oral health that tracks over time and can predict potential problems ahead. These tools use X-ray and other digital imaging technology to provide secondary review and analysis of patient health. Some examples:
Improving case acceptance through AI visualization. Dmitry Tuzoff, the CEO of Denti.ai, a company focused on automated diagnostics and charting for dental X-rays, CBCT and voice data, believes there are two main problems practitioners need to fix: the rate of patient acceptance and the rate of patient compliance. Patient acceptance is largely a function of trust, he says, and the challenge to doctors is how to generate greater trust. One solution his company and others (including Overjet) are working on is to create better 2D and 3D imaging that help patients clearly understand and see what’s happening in their mouth. The best software will also predict what will happen in the future—helping patients understand, for example, that a simple filling now will save them from a root canal (or worse) down the road.
Improving case acceptance through self-tracking. The second major issue Tuzoff and his team are working on concerns patient compliance. This, he says, is based on his findings that just two-thirds of Americans go to the dentist twice a year. To improve this, AI will help doctors target their patients (in a nonintrusive way!) to help them better understand their daily oral health: when to go to the dentist, how urgent their situation is and what their next steps should be. DentalMonitoring, based in Austin, Texas, is perhaps the most consumer-focused of the current dental-AI startups. Its ScanBox digital tool and companion app, which enables lay patients to take high-quality intraoral images at home, is just one way doctors can monitor their patients from afar, and at more frequent intervals than ever before.
Improving case acceptance through longitudinal tracking. For patients who might not initially accept their diagnosis, AI can provide quantitative measures of a patient’s progression (e.g., bone loss), as well as compelling visualizations of that progression. This provides doctors with evidence to support a call for care escalation and encourage patient compliance. Once treatment is chosen, doctor and patient can continue to monitor and track their health over time—helping monitor marginal integrity, bone restoration and more.
Improving case acceptance through reduction in insurance friction. A more prosaic, less futuristic AI application is getting over the final case-acceptance hurdle of insurance claims, billing and patient management. Many AI startups therefore focus on streamlining back-office management through improvement of patient records, correspondence and insurance claims.
Improving case acceptance through reduction in insurance friction. A more prosaic, less futuristic AI application is getting over the final case-acceptance hurdle of insurance claims, billing and patient management. Many AI startups therefore focus on streamlining back-office management through improvement of patient records, correspondence and insurance claims.
Claim reviews are still largely dependent on manual clinical and administrative intervention. This can spark tension between payer and provider, leading to extending processing times, the perception of inconsistency in approvals and denials and, ultimately, delayed benefit payments for the patient.
Clinicians also struggle with insurers and the burden of proof necessary to defend their care scenarios. However, AI will
increase the precision of insurance guidelines and can quantify what is required to support data-driven clinical review. In the not-distant future, dentists who incorporate AI will be better able to understand claim submissions and when additional clinical evidence may be needed.
At the same time, insurers will be able to use AI to speed up manual review, better detect fraud, waste and abuse, and to more clearly share treatment preapproval. Both traditional insurers (Delta Dental) and upstarts (Beam Dental, out of Columbus, Ohio) are working to incorporate AI into their coverage.
AI in the Daily Practice
In addition to providing care, of course, dentists often manage their practice’s operations as well. This includes oversight of quality control among providers and maintaining standards of care and regulatory compliance. AI models configured to one’s specific business and clinical goals can monitor patient data over time. This enables the software to flag opportunities for improvements related to incorrect documentation, missed treatments and compliance with office protocols, improving patient care and the practice’s reputation over time.
In a review of AI applications across dental practices published in the May 2021 issue of the Journal of the Canadian Dental Association, researchers showcased how the technology can significantly improve clinical findings in virtually every major area of dentistry:
 Radiology: Convolutional neural networks have demonstrated a precision rate of 95.8 to 99.5 percent in detecting and identifying teeth, almost rivaling the work of human experts, whose precision rate was 99.9 percent. In 3,000 periapical radiographs of posterior teeth, a CNN algorithm was able to detect lesions at an accuracy of 75.5 to 93.3 percent—a considerable improvement over diagnosis by clinicians using radiographs alone, whose sensitivity varied from 19 to 94 percent.
Radiology: Convolutional neural networks have demonstrated a precision rate of 95.8 to 99.5 percent in detecting and identifying teeth, almost rivaling the work of human experts, whose precision rate was 99.9 percent. In 3,000 periapical radiographs of posterior teeth, a CNN algorithm was able to detect lesions at an accuracy of 75.5 to 93.3 percent—a considerable improvement over diagnosis by clinicians using radiographs alone, whose sensitivity varied from 19 to 94 percent.
Orthodontics: Artificial neural networks can aid in clinical decision making, helping determine the need for tooth extraction before orthodontic therapy in some patients. Research on four constructed ANNs showed accuracy of 80 to 93 percent in determining whether extractions were needed to treat patients’ malocclusions.
Periodontics: One ANN was 90 to 98 percent accurate in classifying patients as having aggressive or chronic periodontitis. The study concluded that ANNs can be used for accurate diagnosis of such cases using relatively simple, conveniently obtained parameters such as leukocyte counts in peripheral blood.
Oral pathology: Convolutional neural networks have been shown to be a promising aid to diagnosis of head and neck cancer lesions. With specificity and accuracy at 78 to 81.8 percent and 80 to 83.3 percent, respectively (compared with those of specialists, which were 83.2 and 82.9 percent, respectively), CNNs show great potential for detecting tumors in tissue samples or on radiographs.
In short, AI is not going to become a significant part of dentistry in 2022; it’s already being tested in every aspect of the dental practice and is certain to scale to power more applications, more ideas and more innovations. What might that look like?
It’s years away from widespread use in a clinical setting, but the feasibility study is a good first step for dental patients.” —Alex DaSilva
Looking Ahead: Trust but Verify
The future is one in which technology helps dental insurers, practitioners and patients have better control over oral health than they do today. The next five to 10 years in particular may include developments that can help patients more easily pinpoint their pain, for example, or help doctors detect cancer well before invasive surgery might be needed.
 One area in which we can expect continued improvement is within diagnostics, but this will require large-scale advances in X-ray technology: higher-quality images, a better patient experience and lower levels of radiation. Overjet’s Inam believes that’s possible within the next decade.
One area in which we can expect continued improvement is within diagnostics, but this will require large-scale advances in X-ray technology: higher-quality images, a better patient experience and lower levels of radiation. Overjet’s Inam believes that’s possible within the next decade.
The future will also likely include tools like CLARAi (Clinical Augmented Reality and Artificial Intelligence). Developed by researchers at the University of Michigan, CLARAi helps clinicians “see” and map patient pain in real time through special augmented-reality glasses. “It’s years away from widespread use in a clinical setting, but the feasibility study is a good first step for dental patients,” says Alex DaSilva, associate professor at the UM School of Dentistry and director of its Headache and Orofacial Pain Effort Lab.
Another potentially exciting application comes from Dr. Javier Jo, a professor at the University of Oklahoma’s School of Electrical and Computer Engineering and a member of OU Medicine’s Stephenson Cancer Center. He’s developing a new medical device that can detect cancer at early stages, when survival rates are much higher. Dr. Jo’s research involves creating a handheld endoscope to look for precancerous and cancerous lesions in the mouth—and, crucially, “training” it to recognize patterns and signatures of those lesions with great accuracy. “When oral cancer is diagnosed early, treating the patient is much more effective and a lot less invasive,” Dr. Jo says. “The survival rate and the patient’s quality of life
is fairly high.”
For her part, Inam argues that “dental practices have been focused solely on the mouth,” but the future she envisions is one in which better data ownership and data understanding enables dentistry to build on current trends and increasingly be integrated into the practice of whole-body medicine.
WHAT’S HOLDING AI BACK?
Why, with so much promising technology being developed, has AI not seen more widespread adoption by dentists overall? Three factors: a lack of clinical research on specific products; practical questions about AI’s value, usefulness
and ethics; and limited data availability.
Much of the lack of clinical research is based on access to data—itself a function of many practices having incomplete records and an understandable reluctance to share even anonymized patient records. Lack of consistency makes it much harder to study and train AI models, which need literal millions of data inputs to begin to understand and develop analytic and predictive capabilities
Lack of clinical evidence leads to complex questions about AI’s utility. This may involve fear over the safety of one’s patient data, the potentially unethical use of that data and even dentists’ job security and stability. These questions are hardly unique to dentistry and are topics of urgent discussion in nearly every industry as AI marches inexorably forward.
At least 45 ethical issues related to the use of AI in dentistry were noted in 22 studies concerning prudence, equity, privacy, responsibility, democratic participation and solidarity.” —The Journal of Clinical Dentistry
Dentists are right to have questions. A July 2021 research review in the Journal of Clinical Dentistry noted that “at least 45 ethical issues related to the use of AI in dentistry were noted in 22 studies (12.4 percent) concerning prudence, equity, privacy, responsibility, democratic participation and solidarity. Studies rarely mentioned whether an ethical board approval was involved and never cited AI ethics–related guidelines. The frequency of studies mentioning ethical issues related to AI has not increased since 2015 and remains low, indicating a potential lack of interest in the topic. As promising as AI applications in dentistry are, most of the studies analyzed did not share the code developed for algorithms, preventing external replication and raising concerns about how transparent and reproducible AI-related research is in dentistry.”
Industry organizations such as the Dental AI Council and the Association for the Advancement of Medical Instrumentation (AAMI) will be necessary to push for transparency, ensure ethical balance and develop guidance on how and when to incorporate AI into everyday dentistry. The FDA, meanwhile, which is focused on ensuring the ethical and necessary use of clinical AI, just last year approved Overjet as the first “AI Dental Assist” product for the U.S. market.
“We’re seeing dental AI software perform at the level of a team of trained dentists with accuracy closer than the width of a needle,” says Dr. Chris Balaban, Overjet’s clinical director. “These tools unlock the ability to track the progression of disease for each tooth and make the case for evidence-based treatment, supported by unbiased software and clear visuals for patients.”
Guidance for the future incorporation of AI and dentistry should follow the general guidelines currently being normalized within AI practices across all fields. These include the belief that any AI application must illustrate a tangible value such as increased efficiency, safety or quality of care. It must do so while highlighting how individual privacy, patient rights and autonomy are to remain front and center. Finally, these solutions must also highlight and promote trustworthiness in their products via implementation of continuous human oversight and evidence-based standards.
Practitioners, professional boards and industry ethicists all must make every effort to employ explainable AI—that is, software that can share its data-input methods and reasoning, and to educate consumers about how AI is being used, and why. Following these practices will ensure continued advances in patient health while abating concerns about this admittedly strange, rapidly scaling technology that will transform dentistry in ways uncountable in the years and decades ahead.
KRISTINA LIBBY (kristina libby.com) is a writer based in New York City. Her work has appeared in the Boston Globe, Popular Mechanics, Elle and more. This is her first piece for Incisal Edge.